The outcomes from cardiorespiratory arrest, even with resuscitation, are poor. Of those children who do survive many are left with neurological deficits.
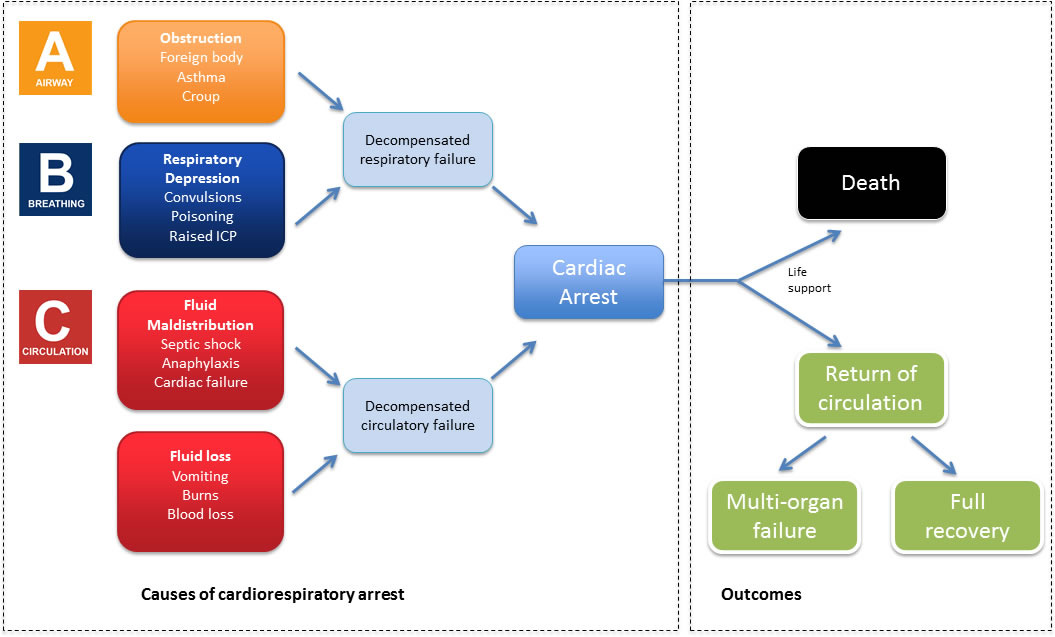
For the majority of children who suffer cardiorespiratory arrest the cause is hypoxic in origin (see figure below). Therefore the priority is prompt oxygenation which is provided by 5 initial rescue breaths.
The most common cardiac arrhythmia is profound bradycardia. This can then deteriorate into asystole and full cardiorespiratory arrest. Again the priority is good oxygenation and BLS rather than defibrillation.
There are a small number of children who have primary cardiac conditions and enter primary cardiac arrest (e.g. ventricular fibrillation (VF) or pulseless ventricular activity (PEA). In these cases early defibrillation, e.g. with an AED, can lead to optimal outcome, however these cases are rare.
Understanding the causes of cardiorespiratory arrest in children is not only important for understanding why paediatric BLS follows a different algorithm. As discussed the outcome is poor. Therefore early recognising and responding to children who are unwell using an ABCDE approach can prevent arrest and therefore prevent morbidity and mortality.