An epileptic seizure occurs as a result of abnormal electrical activity in the brain. Convulsions are the motor signs of this electrical discharge. There are many different types of seizures, which broadly can be divided into
Common causes in childhood include fever (in children under the age of 6 years), head injury, hypoglycaemia, other metabolic abnormalities, hypoxia, epilepsy, meningitis, and drug ingestion
When managing a patient who is experiencing a seizure ensure the patient is not in a position where they are going to injure themselves further. Do not actively restrain them.
Broadly the management of seizures is directed at keeping the patient safe during convulsive activity, controlling the seizures pharmacologically and treating the cause.
The key to successful management is to maintain an ABCDE approach and not focus to greatly on the seizure itself.
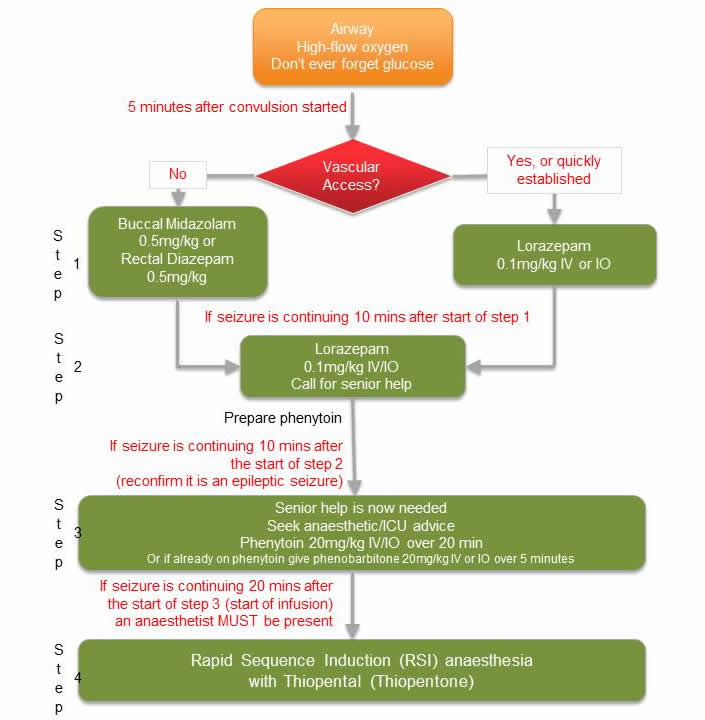
Benzodiazepines such as lorazepam, midazolam or diazepam are used to terminate seizure activity followed by drugs such as phenytoin or phenobarbitone in resistant cases. Early anaesthetic involvement is important if the patient does not respond to initial measures or enters status epilepticus (seizure lasting > 30 minutes). The management of status epilepticus is outlined in the medical emergencies section.
Hypoglycaemia is a common and rapidly reversible cause of reduced conscious state. Blood glucose levels <4 mmol/L warrant treatment.
In a conscious patient, sugary snacks or ‘hypostop’ gel can be given. Even in an unconscious patient, ‘hypostop’ gel can be rubbed into the buccal mucosa where it is rapidly absorbed and does not represent a significant risk of aspiration. If intravenous access is established then give 2 mls/kg 10% dextrose as a bolus and follow this up with an infusion containing glucose as rebound hypoglycaemia can occur. If the patient is critically ill then glucagon intramuscular (IM) can be used which may be found in the crash trolley. It is important to recheck blood glucose levels regularly in someone with a history of hypoglycaemia and ensure they receive subsequent energy source to prevent further hypoglycaemic episodes. If hypoglycaemia is a new condition in the patient then blood should be taken for a hypoglycaemia screen.
Meningitis is an inflammation of the meninges usually caused by either viral or bacterial infection. Viral meningitis can be preceded by an upper respiratory tract infection or a gastroenteritis. Bacterial meningitis is most commonly caused by Group B Streptococcus in neonates and by Neisseria Meningitidis in other age groups. The incidence of meningitis has decreased since the introduction of the HiB vaccine as Haemophilus Influenza used to be a common causative organism. The mortality and morbidity from bacterial meningitis remains high and for this reason prompt recognition and treatment can be life-saving.
The signs of meningitis can vary considerably; older children may have fever, neck stiffness, vomiting, headache and photophobia but these are rarely seen in babies and younger children. In this age group signs suggestive of meningitis include: drowsiness, high-pitched cry, irritability, apnoeic episodes, seizures, fever with no obvious focus, poor feeding, rash (may be blanching or purpuric). A bulging fontanelle is a late sign and in most cases is not present. A diagnosis can be confirmed by analysis of CSF from a lumbar puncture and treatment includes antibiotics. In neonates we treat with a penicillin and gentamicin and in older children we use a broad spectrum antibiotic; usually either cefotaxime or ceftriaxone.
In situations where you are considering lumbar puncture it is also imperative to consider whether lumbar puncture is contraindicated.
Contradictions to lumbar puncture: A lumbar puncture should not be performed in a child with any of the following (LUMBAR SPINE acronym), as they are suggestive of intracranial pathology:
When a lumbar puncture is performed CSF is sent for microscopy culture and sensitivity, protein, glucose, PCR for herpes simplex encephalitis and other viruses (depending on clinical suspicion).
Opioid overdose is a common reason for a reduced conscious level. It can be a deliberate overdose (self harm) or accidental due to an administration error. It is also possible that normally safe doses of opioids can result in serious side effects if there is a decrease in kidney function as this leads to a reduced excretion of the drug and its metabolites. Other signs of an opioid overdose include a depressed respiratory rate and pin point pupils. An opioid overdose is reversed with naloxone, which is an opioid receptor antagonist. Benzodiazepines can also cause a reduced GCS, which can be treated with flumazenil.