The chest x-ray (CXR) is the most common imaging performed in children. Having a good system for interpreting the findings will reduce the chance of you missing pathology
| Quality of the film | R Rotation | • Verify equal distance between medial ends of clavicles and vertebral spinous process OR equal length of clavicles |
| I Inspiration | • The chest is well inspired if there are 9 posterior (or 6 anterior) ribs visible above the mid-diaphragm. | |
| P Penetration | • The radiograph is normally penetrated if vertebral bodies are just visible through the cardiac shadow. | |
| Evidence of pathology | A Airway | • Trachea central between the ends of the clavicles. |
| B Bones | • Start at each corner of the CXR and work inwards. Note any fractures and quality of the bones. | |
| C Cardiac Silhouette | • Review: Heart size (PA film <0.5 cardiothoracic ratio), borders and shape | |
| D Diaphragm | • Identify costo-phrenic and cardio-phrenic angles; these should be sharp and clear. | |
| E Edges and External soft tissues | • Check the edges for pneumothorax (free air). • Look at the external soft tissues including breast shadows |
|
| F Fields | • Look at both lung fields and apices. Compare each side for differences in density. • Assess for lung fissures, vascularity, nodules, consolidation and masses. |
|
| G Gastric bubble | • Check for lucency in the left upper abdominal quadrant. | |
| H Hilum | • Enlargement may appear as a widened mediastinum. Calcification (appears white), can due to previous TB. | |
| I Insertions/ Artefacts | • Check for artifacts e.g. naso-gastric (NG) tubes, central lines, tracheal tubes and other medical equipment or clothing. |
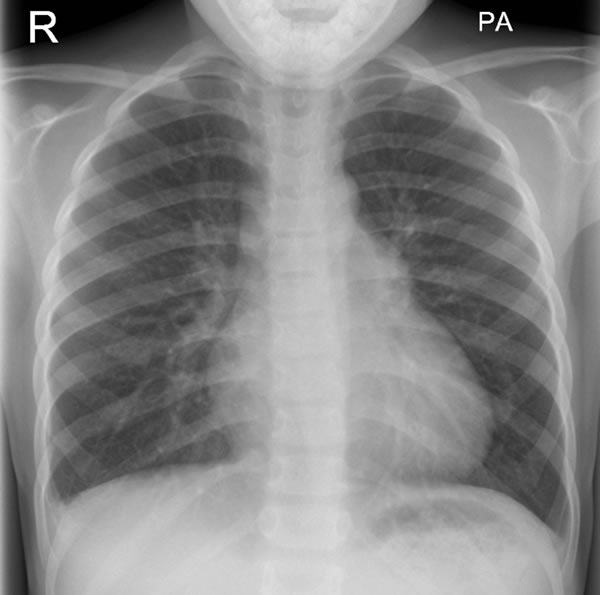
Case: 5-year-old presented with 4 days history of cough and increased work of breathing. He also developed temperature since last 3/7 days, which is not responding to regular antipyretics.

Case 1 interpretation

Conclusion: Consolidation in left lower zone representing a left lower pneumonia and likely effusion
Case: 5 year old presented with one week history of cough and increased work of breathing. She also developed temperature since last 3/7 days, which is not responding to regular anti pyretics. Auscultation of her chest reveals bilateral crackles at bases.

Case 2 interpretation

Conclusion: Bilateral mid and lower zone opacity likely to represent bilateral, lower-lobe, pneumonic changes
10 year old boy was seen by GP with history of increased temperature, cough and increased respiratory rate. He was treated with oral antibiotics. He presented to A&E with worsening of symptoms and respiratory distress after completing course of antibiotics.

Case 3 interpretation

Conclusion: right mid and lower lobe consolidation with left sided effusion
10 year old boy presented with sudden onset of shortness of breath and severe chest pain following road traffic accident. Examination of chest revealed reduced air entry on left side with hyper resonant percussion note on left.
Case 5 interpretation

Case 4 interpretation

Conclusion: left sided pneumothorax
3 month old presented with 48 hours h/o reduced feeding and increased work of breathing. His chest revealed tachypnoea with bilateral recessions and fine inspiratory crackles.
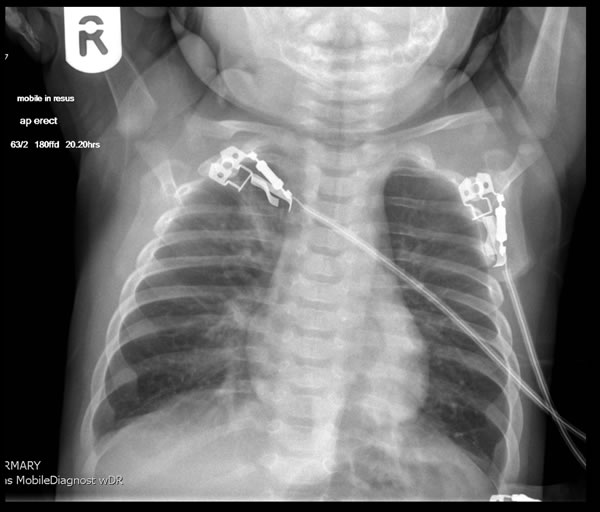
Case 5 interpretation

Conclusion: Indeterminate chest radiograph. Clinical features consistent with bronchiolitis