There are two basic airway manoeuvres that should be tried when managing an obstructed airway;
These are particularly useful when the cause of the obstruction is reduced consciousness and loss of the pharyngeal tone. These are also the techniques used in BLS and are discussed in more details in the respective BLS chapter.
It is important also to check for any foreign bodies. If there is an obvious foreign body which can easily be removed this should be done under direct vision. Do not attempt a blind finger sweep.
There are often lots of oral secretions which can partially obstruct the airway. A large bore suction device (such as a Yankaur) can be used to remove these. Again, this should be done under direct supervision (see image above)
The oropharyngeal airway or 'Guedel' airway is designed to be used in patients with a reduced conscious level to overcome the soft palate obstruction by preventing the backward displacement of the tongue. They are available in different sizes (2, 3 and 4 most common).
Caution should be used in patients who are only lightly unconscious, as they may not have lost their laryngeal reflexes enough to tolerate an oropharyngeal airway, and gagging or laryngospasm may be triggered.
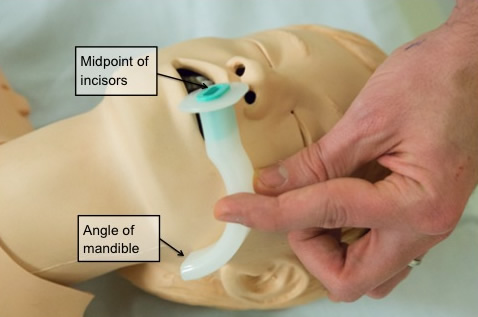
In children and infants the oropharyngeal airway must be inserted as it would sit in the airway (with the end pointing downwards). In older children it can be inserted as in adults.
The nasopharyngeal airway (NPA) is made from soft plastic, bevelled at one end and flanged at the other. It is inserted through the nose, perpendicular to the hard palate, with a slight twisting action, until the tip lies in the posterior pharynx. It is better tolerated than the oropharyngeal airway in patients who are not deeply unconscious. Because of a high incidence of bleeding/epistaxis after insertion they are generally best reserved for patients who do not tolerate an oropharyngeal airway. They are of use in patients whose mouths cannot be opened (such as in patients with seizures). They are contraindicated in patients with fractures of the base of the skull.
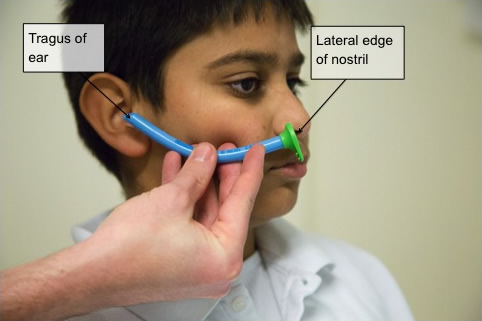
An appropriate diameter NPA is first estimated by finding an NPA the same diameter as the patients little finger, this should then fit comfortably into the nostril without causing sustained blanching of the nostril. The appropriate length of a nasopharyngeal tube is estimated by measuring between the lateral edge of the nostril to the tragus of the ear. If an appropriately sized NPA is not available then a shortened endotracheal tubes may be used.