Reservoir mask. This is also known as a non-rebreathe mask and needs to be connected to a supply of oxygen at 15 L/min.
Basic airway manoeuvres: Head tilt with chin lift or jaw thrust
Remove obvious foreign bodies or suction secretions
This is a demonstration of the use of a Yankauer suction catheter to clear secretions from the mouth. Be careful not to stimulate the oropharynx in a patient with an intact gag reflex as this can provoke vomiting or laryngospasm.
Airway adjuncts
Basic airway adjuncts
including nasopharyngeal and oropharyngeal airways.
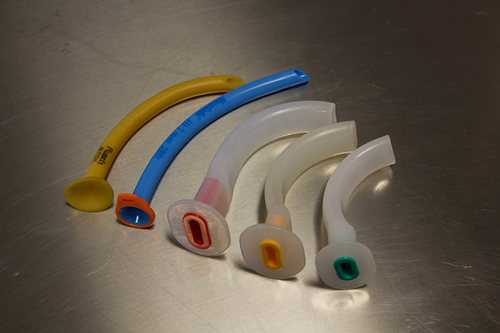
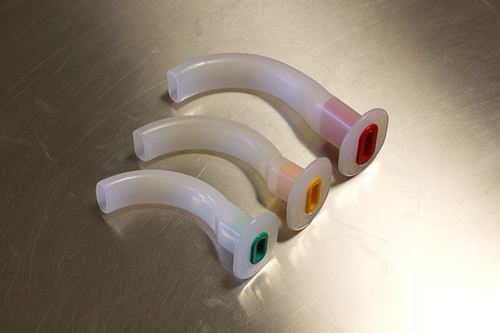
Oropharyngeal airway
Oropharyngeal ‘Guedel’ airways
of different sizes.
Nasopharyngeal airway
Nasopharyngeal airway - these are contraindicated in base of skull fracture
Supraglottic Airway Device and igels
Supraglottic Airway Device and igels
If the patient is not breathing- ventilate using a self-inflating bag and mask e.g. an AMBU bag. Throughout this book the self-inflating bag and mask will be referred to as the “bag and mask” as this is the name most often used clinically.
Bag and mask.
Reduced conscious level:
If the patient is unable to protect their own airway, i.e. they are too
unconscious to cough or gag appropriately then a definitive airway
(endotracheal tube) will be required. A GCS less than 9 or a rapidly falling level of consciousness is an indication for a definitive airway. Call for anaesthetic help.
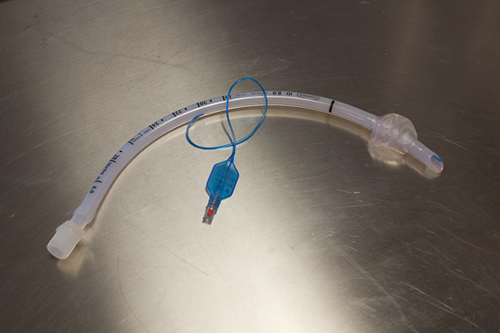
Endotracheal tube. This is an endotracheal tube with the cuff inflated. The blue pilot balloon with a one-way valve is visible to which an air filled syringe is connected to inflate the cuff. When in situ in the trachea with the cuff inflated this forms a 'definitive airway', and enables the patient to be ventilated whilst protecting the airway from gastric content and other secretions that may track down from the upper airway in an unconscious patient.
Anaphylaxis:
A broad range of antigens found in food, drugs and other substances, can trigger anaphylaxis. There is a variable clinical presentation but it is normally characterised by a rapid deterioration with rash and life threatening airway, breathing and circulatory problems.
There can be airway swelling (tongue, mucous membranes and pharynx), which can manifest as difficulty breathing and swallowing secondary to laryngeal oedema and bronchospasm. A hoarse voice or stridor may be evident. Like with any acute patient deterioration, life threatening airway problems need to be dealt with prior to breathing and circulatory problems.
A full description of management of anaphylaxis can be found elsewhere but management includes; calling for help, removal of the trigger, intramuscular or intravenous adrenaline, maintaining airway patency (intubation may be necessary) and management of bronchospasm and cardiovascular collapse.
Upper image - Emergency drug box usually found on 'crash' trolleys and in other acute areas. Lower image - adrenaline minijet and ampoules.
Epiglottitis:
Epiglottitis is inflammation of the epiglottis, which as a consequence can enlarge and cause airway obstruction. This most often is caused by a bacterial infection and affects children more than adults. The incidence has decreased since the introduction of the Hib vaccine against haemophilus influenza. The management of this medical emergency includes treating the underlying cause with antibiotics.
Supraglottitis:
Supraglottitis is inflammation of the supraglottic structures, which again causes swelling and potential airway obstruction. The management of these medical emergencies include protecting the airway with an endotracheal tube placed by an experienced anaesthetist and treatment of the underlying cause with antibiotics.